
Tags
Is there a cure for the common cold yet? No?
Then what do you do when you get a common cold? The flu? You stay home, rest, drink lots of liquids, and hope your grandma, wife or husband, or other family member fixes you some hot chicken soup. Sometimes you get the chills and sometimes it’s hard to breathe because your nose is stopped up and you have congestion in your chest, and you welcome the steam vapors from the hot soup. You cough and feel pretty lousy for a few days to a week and then you begin to feel better. Within two weeks, you are back to normal, ready to go outside and play or go back to work.
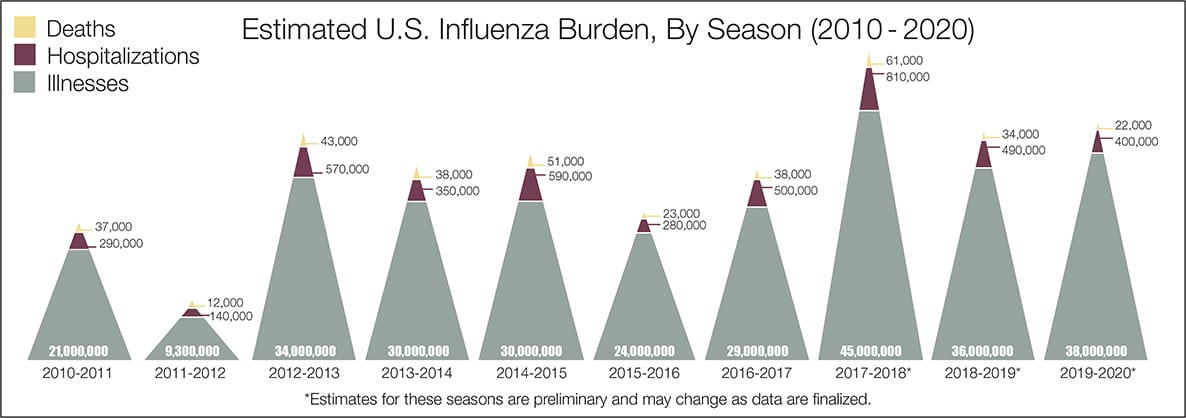
Have people died of the common cold or flu? Yes, of course, they have. There’s a record of that here: https://www.cdc.gov/flu/images/about/burden/influenza-burden-chart2-960px.jpg

Notice the death count as opposed to the illness count. Notice the years where the death count is higher than in the year 2020. Notice the ratios between the illness count and death count. Example:
2010-2011 Illness count 21 million; death count 37 thousand
2011-2012 Illness count 9.3 million; death count 12 thousand
2012-2013 Illness count 34 million; death count 43 thousand
2013-2014 Illness count 38 million; death count 38 thousand
2014-2015 Illness count 38 million; death count 51 thousand
2015-2016 Illness count 24 million; death count 23 thousand
2016-2017 Illness count 29 million; death count 38 thousand
2017-2018 Illness count 45 million; death count 61 thousand
2018-2019 Illness count 36 million; death count 34 thousand
2019-2020 Illness count 38 million; death count 22 thousand
(You might think of the Illness count sort of like the Covid-19 Case counts except with case counts no one is ill. It just means the PCR test – which does not test for a virus – is positive for something but that something is only positive after 37-40 exponential amplifications. In other words, a positive PCR test is meaningless.)
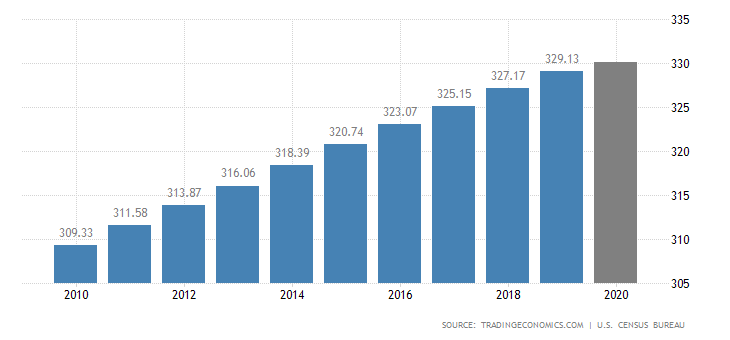
To make sense of these numbers, the population needs to be factored in. https://tradingeconomics.com/united-states/population
Also, there have been other pandemics in our history so they need to be looked at too
https://www.worldatlas.com/articles/10-pandemics-throughout-history.html

To continue comparing apples to apples, we should begin with the year 2010 to 2020 – but there aren’t any except for covid-19. But let’s look at other pandemics from the website anyway to see how death rates compared and also to see if the world was shut down because of those rates. And, of course, we must assume that every word in the listed pandemics is true unless you do some digging and then you will find that much of it also has strange back-stories. But I digress from the point of this post.
1. COVID-19 Pandemic 2019 – The symptoms they claim are respiratory symptoms, fever, coughs, shortness of breath, difficulties in breathing, and add, but those symptoms could also mean you have a common cold or the flu.
2. SARS (2002-2004) – It infected 8,098 people worldwide and killed 774 people.
3. HIV/AIDS (1981) – Infected more than 65 million people worldwide.
4. H3N2 Pandemic (1968) – It killed an estimated one million people.
5. Spanish Flu (1918-1919) – Infected 1/3 of the world’s population and killing 20 to 50 million people worldwide.
6. Russian Flu of 1889 (1889-1890) – An estimated 1 million people died.
7. Cholera (1871-1824) – Not a virus but it’s listed as a pandemic…
8. Small Pox Pandemic (1870-1874) – Killed three out of ten victims. Caused 500,000 deaths worldwide.
9. The Black Death (1347-1352) – Killed an estimated 25 million people in Europe.
10. Antonine Plague (165 AD-180 AD) – Killed 2,000 people per day.
The world was not shut down for any of these except #1.
Wait a minute. What happened to Zika, Swine flu, Ebola, MERS, SARS, H1N1, H1N5, and so on? It’s very interesting that after all the hype and hoopla about these pandemics, they didn’t make it to the list above. Maybe they are best forgotten as flopped attempts to scare people into isolation. https://wakeup-world.com/2016/04/06/ebola-swine-flu-zika-sars-the-anatomy-of-a-false-flag-disease/
WITH STATS LIKE THIS WHY DID WE SHUT DOWN THE WORLD this time?

THERE MUST BE SOME OTHER REASON…
OMG, there is!

WHO Memos 1972 Explains How To Turn Vaccines Into A Means Of Killing
https://thebridgelifeinthemix.info/health/who-memos-1972-explains-how-to-turn-vaccines-into-a-means-of-killing
TIME TO TAKE ACTION TO STAY ALIVE:
Everyone can stop wearing their masks. They can stop social distancing. They can stop being in fear of dying of a virus (that doesn’t even exist). They don’t need to take the gates vaccine (that will turn them into the equivalent of robots or kill them). They can go back to work, open their shops; go to restaurants, movies, social events. They can be with their families and friends again. They can start living again.
If a police officer tries to stop you, well he or she doesn’t know the danger that never existed has ended. You can give them the pie chart above. You can tell them you won’t obey. You won’t comply. The rule is stupid. The rule harms others rather than protect others. The rule has no authority because you don’t give it any authority. The rule is unconstitutional and not lawful.
“Such childish excitement over a common cold suggests the entire event is a show to cover one or more real events the elect want hidden. We have two choices: either it is the cover for the financial reset or a cover for the symptoms created by the hiking up of the 5G frequencies. It could also be a cover for both.” OR… it could be something completely different, like the Great Reset, thanks to Klaus Schwab.
You don’t think covid-19 equates to the common cold or flu? Well, have a look at what Dr. Anthony Fauci says to doctors but not the white house:
Fauci wrote an editorial to the New England Journal of Medicine on February 28th stating that this pandemic is akin to seasonal flu. Then in the white house, he told the president to keep the lockdown going another month after month after month (see highlighted statement below).
https://www.nejm.org/doi/full/10.1056/NEJMe2002387?fbclid=IwAR2eIUdwdFM5pZ_mQ1sCN_GMFWNgW9oNJF0RiXXtfJRn4pukHGWsP3PYStk
The latest threat to global health is the ongoing outbreak of the respiratory disease that was recently given the name Coronavirus Disease 2019 (Covid-19). Covid-19 was recognized in December 2019. 1 It was rapidly shown to be caused by a novel coronavirus that is structurally related to the virus that causes severe acute respiratory syndrome (SARS). As in two preceding instances of emergence of coronavirus disease in the past 18 years 2 — SARS (2002 and 2003) and Middle East respiratory syndrome (MERS) (2012 to the present) — the Covid-19 outbreak has posed critical challenges for the public health, research, and medical communities.
In their Journal article, Li and colleagues 3 provide a detailed clinical and epidemiologic description of the first 425 cases reported in the epicenter of the outbreak: the city of Wuhan in Hubei province, China. Although this information is critical in informing the appropriate response to this outbreak, as the authors point out, the study faces the limitation associated with reporting in real-time the evolution of an emerging pathogen in its earliest stages. Nonetheless, a degree of clarity is emerging from this report. The median age of the patients was 59 years, with higher morbidity and mortality among the elderly and among those with coexisting conditions (similar to the situation with influenza); 56% of the patients were male. Of note, there were no cases in children younger than 15 years of age. Either children are less likely to become infected, which would have important epidemiologic implications, or their symptoms were so mild that their infection escaped detection, which has implications for the size of the denominator of total community infections.
On the basis of a case definition requiring a diagnosis of pneumonia, the currently reported case fatality rate is approximately 2%. 4 In another article in the Journal, Guan et al. 5 report mortality of 1.4% among 1099 patients with laboratory-confirmed Covid-19; these patients had a wide spectrum of disease severity. If one assumes that the number of asymptomatic or minimally symptomatic cases is several times as high as the number of reported cases, the case fatality rate may be considerably less than 1%. This suggests that the overall clinical consequences of Covid-19 may ultimately be more akin to those of severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.2
The efficiency of transmission for any respiratory virus has important implications for containment and mitigation strategies. The current study indicates an estimated basic reproduction number (R0) of 2.2, which means that, on average, each infected person spreads the infection to an additional two persons. As the authors note, until this number falls below 1.0, it is likely that the outbreak will continue to spread. Recent reports of high titers of virus in the oropharynx early in the course of disease arouse concern about increased infectivity during the period of minimal symptoms.6,7
China, the United States, and several other countries have instituted temporary restrictions on travel with an eye toward slowing the spread of this new disease within China and throughout the rest of the world. The United States has seen a dramatic reduction in the number of travelers from China, especially from Hubei province. At least on a temporary basis, such restrictions may have helped slow the spread of the virus: whereas 78,191 laboratory-confirmed cases had been identified in China as of February 26, 2020, a total of 2918 cases had been confirmed in 37 other countries or territories. 4 As of February 26, 2020, there had been 14 cases detected in the United States involving travel to China or close contacts with travelers, 3 cases among U.S. citizens repatriated from China, and 42 cases among U.S. passengers repatriated from a cruise ship where the infection had spread.8 However, given the efficiency of transmission as indicated in the current report, we should be prepared for Covid-19 to gain a foothold throughout the world, including in the United States. Community spread in the United States could require a shift from containment to mitigation strategies such as social distancing in order to reduce transmission. Such strategies could include isolating ill persons (including voluntary isolation at home), school closures, and telecommuting where possible.9
A robust research effort is currently underway to develop a vaccine against Covid-19. 10 We anticipate that the first candidates will enter phase 1 trials by early spring. Therapy currently consists of supportive care while a variety of investigational approaches are being explored. 11 Among these are the antiviral medication lopinavir–ritonavir, interferon-1β, the RNA polymerase inhibitor remdesivir, chloroquine, and a variety of traditional Chinese medicine products. 11 Once available, intravenous hyperimmune globulin from recovered persons and monoclonal antibodies may be attractive candidates to study in early intervention. Critical to moving the field forward, even in the context of an outbreak, is ensuring that investigational products are evaluated in scientifically and ethically sound studies. 12
Every outbreak provides an opportunity to gain important information, some of which is associated with a limited window of opportunity. For example, Li et al. report a mean interval of 9.1 to 12.5 days between the onset of illness and hospitalization. This finding of a delay in the progression to serious disease may be telling us something important about the pathogenesis of this new virus and may provide a unique window of opportunity for intervention. Achieving a better understanding of the pathogenesis of this disease will be invaluable in navigating our responses in this uncharted arena. Furthermore, genomic studies could delineate host factors that predispose persons to the acquisition of infection and disease progression.
The Covid-19 outbreak is a stark reminder of the ongoing challenge of emerging and re-emerging infectious pathogens and the need for constant surveillance, prompt diagnosis, and robust research to understand the basic biology of new organisms and our susceptibilities to them, as well as to develop effective countermeasures.
Disclosure forms provided by the authors are available with the full text of this editorial at NEJM.org.
This editorial was published on February 28, 2020, at NEJM.org. (emphasis red font added)
It’s up to you in the end. But I will say one thing, or better yet, I concur with what James Corbett said today in this video:
What NO ONE is Saying About The Lockdowns
https://lbry.tv/@corbettreport:0/aboutlockdowns:2
Meanwhile, coronavirus has been patented.
https://thebridgelifeinthemix.info/health/coronavirus-isolated-humans/
(1) it has not been isolated, even though it says it has been
(2) it’s illegal to patent something from nature
(3) if it’s not from nature, then it is biowarfare which is also illegal
(4) either way, all of it is unlawful
And dangerous 5G rolls out unnoticed.
It isn’t a hopeless situation though.
All of this manipulation can be stopped. Not by a shooting war. Not by any sort of violence. It can be stopped by NON COMPLIANCE. By calling your fear a lie. By refusing to obey unlawful rules that are not laws. Even if they were laws, if they are unlawful, they are null and void by the Constitution.
Remember, you are a spirit-being entangled in your physical body. You are made with LOVE. You ARE love. We have been invaded by evil dark side entities. I’ve written about this before (see previous articles in this blog). Re-read the “That’s A Lie program” and set that tool into action now. You won’t be sorry. STOP COMPLYING. Take off your mask, hug your neighbor and friends; break the chains that are holding you in fear; live your life and walk in freedom.
There is no virus.
| The CDC document is titled, “CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel.” It is dated July 13, 2020. Buried deep in the document, on page 39, in a section titled, “Performance Characteristics,” we have this: “Since no quantified virus isolates of the 2019-nCoV are currently available, assays [diagnostic tests] designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA…” The key phrase there is: “Since no quantified virus isolates of the 2019-nCoV are currently available…” Every object that exists can be quantified, which is to say, measured. The use of the term “quantified” in that phrase means: the CDC has no measurable amount of the virus, because it is unavailable. THE CDC HAS NO VIRUS. |
This pandemic really is a scam.
News media outlets, scientists, doctors, and governments are really lying to you. About everything. Wake up! Smell the roses, the coffee, the tea, whatever but wake the heck up. For your sake. For my sake. For the sake of your children and grandchildren. For the sake of humanity and life on planet Earth.
With love to all,
Sherry
http://www.keyholejourney.com

{kind=link}
Great research Sherry, I am forwarding this.
LikeLiked by 1 person
Thank you, Aaron.
LikeLiked by 1 person
Really enjoyed show w/Robert. I’m also from Bay Area. I disagree about there being no virus. 1. It came from lab. 2. It is an evil plot. 3. It is easy to prevent & cure.https://youtu.be/93jI7Gl3yic Sky News Australia Dr. Thomas Borody. He takes IVERMECTIN for prevention,as do I. The powers that be are covering up this cheap,generic & safe solution. We could end the lockdown w/o vaccines asap. If you can’t watch video, I hope you can read & research otherwise I liked your talk, will try to follow your work.
Cheers
Joe
LikeLiked by 1 person
Hi Joseph. Thank you for your comment. I watched the video with Gastroenterologist Professor Thomas Borody. It is interesting. Yes, of course, the cabal balks at anything that is not the gates mRNA vaccine. Any treatment that works goes against their narrative. I’d like to see a conversation between Professor Thomas Borody and Dr. Thomas Cowan, represented here: https://planetwaves.net/planetwaves-fm/
LikeLike
Great hearing you on Robert’s show Sherry! I don’t listen to Robert as much as I used to but must say this is one of the best shows ever. I love your simple approach.
Though I’ve never had luck with any method of relieving the voice/feelings in the many years I’ve been on the journey, I’m going to give your method a go. It’s all so tiresome now. Though I recognize that we are at end game, I often have the fear come over me that December 21st will come and go and we will still be waking up to the same system, not that I believe anything tangible will happen on that date, but it’s kind of nice to believe it possible. It’s a relief to know that someone out there is living a life of peace after having suffered under the thumb of the dark system. Thanks for doing what you do.
LikeLiked by 2 people
Thank you Audrey for your thoughtful words. I am so happy you found the show beneficial. In all my years, I haven’t noticed any special or tangible happenings on a solstice, but I know that others have felt an energy shift. Perhaps it is because my chart is so clumped together, who knows? Actually, I don’t know enough about astrology to speak to this.
I would love to know your progress after using the That’s A Lie program. Caution: be alert to the voices/feelings getting stronger when you first get into the program. That’s a clue that it’s working and they are fighting back to keep you under their spell. Just keep the program going and you will succeed. When the program becomes automatic within you, there is peacefulness and gratitude on the other side for a job well done.
Once that happens, you will see way more clearly than ever before. If you need encouragement, please don’t hesitate to contact me. We do seem to be in the end game which makes it all the more important for each of us to get right with who we are so that we can recognize and learn how to use the internal technology we have each been given. Much love, Sherry
LikeLike
Pingback: WHERE IS EARTH’S TIMELINE GOING? | Keyholejourney Blog - exploring mind-opening concepts